Kỹ thuật di động khớp cổ và bàn tay, phần 1 (các khớp quay- trụ dưới, quay- cổ tay, gian cổ tay).
ANATOMY REVIEW
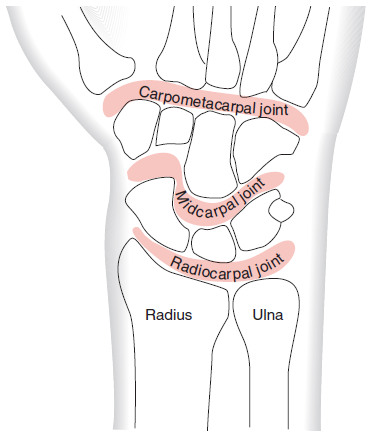
Bones and Joints

Từ vựng:
- Radius: xương quay
- Ulna: Xương trụ
- Ulnar styloid: mỏm trâm trụ
- Carpals: Các xương cổ tay (gồm hai hàng, thuyền nguyệt tháp đậu/thang thê cả móc)
- Metacarpals: Các xương bàn
- Phalangges: Các xương ngón tay
Physiologic (Osteokinematic) Motions of the Wrist and Hand
Các vận động sinh lý (chuyển động học xương) của cổ và bàn tay


Từ vựng:
- Flex: Flexion/ gấp
- Ext: Extension/duỗi
- Add: Adduction, khép ( =nghiêng trụ với cổ tay)
- Abd: Abduction, dạng (= nghiêng quay với cổ tay)
- Supination: quay ngửa
- Pronation: quay sấp
- Volar: mặt lòng, mặt bụng
- Dorsal: mặt mu, mặt lưng
- Distal: đầu xa, đầu dưới
- Proximal: đầu gần, đầu trên
- Radioulnar joint: khớp quay trụ
- Radiocarpal joint: khớp quay cổ tay
- Intercarpal joint: khớp gian cổ tay
- CMC: khớp cổ bàn tay
- MCP: khớp bàn ngón tay
- PIP: khớp liên ngón ngón gần
- DIP: khớp liên ngón xa
- End feel: cảm giác cuối tầm (của khớp)
Accessory (Arthrokinematic) Motions of the Wrist and Hand
Các vận động phụ trợ (chuyển động học khớp) của cổ và bàn tay


Notes/Ghi chú:
- Physiologic Motions: vận động sinh lý, chuyển động xương
- Accessory Motions: vận động phụ trợ, chuyển động học khớp, joint play
- OPP: Open Packed Position/ Tư thế khớp mở = resting position, tư thế khớp nghỉ: là tư thế thường dùng bắt đầu để di động khớp. Ghi nhớ quy luật mặt lồi/lõm
- CPP: Closed Packed Position/ Tư thế khớp khoá
- OKC: open Kinetic Chain: Chuỗi động mở: Kỹ thuật di động khớp thường dùng ở chuỗi động mở để khu trú lên khớp được thực hiện
- Concave: lõm
- Convex: lồi
- Glide: trượt
- Distraction: kéo tách
- Trong kỹ thuật, kỹ thuật viên thực hiện cố định đầu gần/phần xương cố định: Dấu chéo đỏ
- Kỹ thuật viên thực hiện vận động phụ trợ: Mũi tên xanh
- Người bệnh có thể thực hiện vận động sinh lý phối hợp: Mũi tên vàng
XEM THÊM: GIẢI PHẪU CHỨC NĂNG PHỨC HỢP CỔ BÀN TAY. XƯƠNG VÀ KHỚP
DISTAL RADIOULNAR (R/U) JOINT MOBILIZATIONS
Distal R/U Dorsal and Volar Glides/Trượt khớp quay trụ dưới về phía mu và lòng
Indications:
- Nói chung tăng gấp duỗi cổ tay, kèm theo sấp và /hoặc ngửa
- Distal radius on ulna dorsal and volar glides (trượt đầu dưới xương quay lên xương trụ về phía mu và phía lòng): to improve forearm supination and pronation, respectively, as well as wrist flexion and extension.
- Distal ulna on radius dorsal and volar glides (trượt đầu dưới xương trụ lên xương quay về phía mu và phía lòng): to improve forearm pronation and supination, respectively, as well as wrist flexion and extension.
Accessory Motion Technique/Kỹ thuật vận động phụ trợ (mặt khớp)
- Patient Position: sitting position with the forearm supported on the table, or elbow flexed on table with the dorsum of the hand facing the clinician. The wrist may be pre-positioned at the point of restriction.
- Clinician Position & Hand Placement:
- Sit on the ipsilateral side of the wrist being mobilized.
- Sabilization hand: grasp the distal ulna or radius with a lumbrical grip (cầm nắm kiểu giun) over the radial side of the wrist and hand.
- Mobilization hand: Using lateral pinch grasp the distal ulna and ulnar head.
- Force Application:
- For technique 1, while stabilizing the ulna, apply a dorsal or volar glide to the radius for supination and pronation, respectively. While stabilizing the radius, apply a dorsal or volar glide to the ulna for pronation and supination, respectively.
- For technique 2, the thumb places volar force at the ulnar head as the flexed second digit of the mobilization hand is positioned over the pisiform to stabilize the proximal row of carpal bones. The stabilization hand stabilizes the distal radius and radial aspect of the wrist. Alternately, stabilize the radial side of the wrist and hand using a lumbrical grip while the ulna is mobilized volarly against a stabilized triquetrum.


Accessory With Physiologic Motion Technique (Kỹ thuật vận động phụ trợ kết hợp vận động sinh lý)
- Patient Position: sitting or supine position with the elbow flexed to 90 degrees and the forearm in full pronation for volar glides and supination for dorsal glides.
- Clinician Position & Hand Placement:
- Sit on the side ipsilateral to the elbow being mobilized.
- Thumb over thumb contact at the distal aspect of the radius or ulna with the fingers of both hands grasping the wrist to guide the forearm into pronation or supination.
- Force Application: As the patient actively moves from full pronation to full supination or the reverse, maintain a volarly directed or dorsally directed force, respectively. As the patient provides overpressure into supination or pronation, maintain force throughout the entire range of motion and sustain the force at end range. Be prepared to move during the mobilization to ensure correct force application.

RADIOCARPAL (R/C) JOINT MOBILIZATIONS
Radiocarpal Distraction
Indications:
- To improve motion in all directions
Accessory Motion Technique:
- Patient/Clinician: sitting position with the forearm supported by the table, the wrist in neutral, and the hand over the edge of the table. The wrist may be pre positioned at the point of restriction.
- Clinician Position & Hand Placement:
- Sit on the ipsilateral side of the wrist being mobilized.
- Stabilization hand: grasp the distal radius and ulna.
- Mobilization hand: place immediately adjacent to the stabilization hand just distal to the patient’s wrist over the proximal row of carpal bones.
- Force Application: After taking up the slack in the joint, apply force in the direction of the long axis of the forearm.


Accessory With Physiologic Motion Technique
- Patient Position: the same position as described above.
- Clinician Position & Hand Placement: the same as that described above.
- Force Application: As the patient actively flexes and extends the wrist, apply a distraction force. Be prepared to move during the mobilization to ensure correct force application. Force is maintained throughout the entire range of motion and sustained at end range.
Radiocarpal Dorsal and Volar Glides
Indications:
- Dorsal glides to improve wrist flex/trượt về phía mu để cải thiện gấp cổ tay
- Volar glides to improve wrist ext/trượt về phía lòng để cải thiện duỗi cổ tay
Accessory Motion Technique:
- Patient Position: sitting with the elbow flexed to 90 degrees and forearm pronated with the wrist in neutral and the hand over the edge of the table. You may pre-position the patient with the wrist at the point of restriction.
- Clinician Position & Hand Placement:
- Sit on the ipsilateral side of the wrist being mobilized.
- Stabilization hand: grasp the distal radius and ulna.
- Mobilization hand: place immediately adjacent to the stabilization hand just distal to the patient’s wrist over the proximal row of carpal bones.
- Force Application: Take up the slack in the joint, and apply force in an upward direction for dorsal glides and apply force in a downward direction for volar glides.


More pictures:



Accessory With Physiologic Motion Technique (Not pictured)
- Patient Position: the same position as described above.
- Clinician Position & Hand Placement: the same as described above.
- Force Application: As the patient actively flexes the wrist, apply a dorsal glide. As the patient actively extends the wrist, apply a volar glide. Be prepared to move during the mobilization to ensure correct force application. Force is maintained throughout the entire range of motion and sustained at end range.
Radiocarpal Medial and Lateral Glide
Indications:
- Medial & lateral glides to improve RD & UD, respectively
Accessory Motion Technique:
- Patient Position: sitting with her elbow flexed to 90 degrees and her forearm between pronation and supination with her hand over the edge of the table. You may pre-position the patient with her wrist at the point of restriction.
- Clinician Position & Hand Placement:
- Sit on the ipsilateral side of the wrist being mobilized.
- Stabilization hand: Grasp the distal radius and ulna
- Mobilization hand: place immediately adjacent to your stabilization hand, just distal to the patient’s wrist over the proximal row of carpal bones.
- Force Application: Force is applied in a downward direction for medial glides and an upward direction for lateral glide.



Accessory With Physiologic Motion Technique
Patient Position: the same position as described above.
Clinician Position & Hand Placement: the same as described above.
Force Application: The patient actively moves into wrist flexion, extension, radial deviation or ulnar deviation as you apply a medial or lateral glide through the mobilization hand. The patient applies overpressure at end range. Be prepared to move during the mobilization to ensure correct force application. Force is maintained throughout the entire range of motion and sustained at end range.

MIDCARPAL AND INTERCARPAL JOINT MOBILIZATIONS
Midcarpal and Intercarpal Multiplanar Glide
Indications:
- Midcarpal and intercarpal dorsal and volar glides of the proximal row of carpal bones: to improve wrist flexion and extension, respectively.
- Midcarpal and intercarpal dorsal and volar glides of the distal row of carpal bones: to improve wrist extension and flexion, respectively.
- Multiplanar glides: important for intercarpal mobility in all directions.
Accessory Motion Technique
- Patient Position: sitting position with the forearm fully pronated and supported on the table. You may pre-position the elbow at the point of restriction.
- Clinician Position & Hand Placement:
- Sit on the ipsilateral side of the elbow being mobilized.
- Tip-to-tip pinch grasp contacts two adjacent carpal bones.
- Force Application: Force is applied in a dorsal, volar, or multiplanar fashion in the direction of greatest restriction.
Accessory With Physiologic Motion Technique (Not pictured)
- Clinician Position & Hand Placement: the same as described above.
- Force Application: The patient actively performs wrist movement in any direction as stabilization and mobilization contacts are maintained throughout the range of motion and sustained at end range.

INTERCARPAL JOINT MOBILIZATIONS
Intercarpal Volar/Dorsal Glide High Velocity Thrust
Indications:
- to alter positional relationships, breaking through adhesions that may be restricting motion, or
- to facilitate general improvements in mobility at any of the intercarpal joints.
Accessory Motion Technique
- Patient Position: sitting position with the wrist in approximately 20 degrees of flexion with fingers relaxed for volar glides and 20 degrees of extension for dorsal glides.
- Clinician Position & Hand Placement:
- Stand facing the patient
- Both hands grasp the patient’s hand. Thumb over thumb contact is placed on the dorsal aspect of the carpal bone to be mobilized for volar glides and on the volar aspect of the carpal bone for dorsal glides. Fingers wrap around hand and control wrist motion.
- Force Application: From the starting position, the wrist is brought toward extension or flexion, and at end range a short-amplitude, high-velocity thrust is applied in a volar or dorsal direction through the thumb contacts.

References:
- Christopher H. Wise, Dawn T. Gulick. Mobilization Notes: Rehabilitation Specialist’s Pocket Guide. F. A. Davis Company, 2009.
- Christopher H. Wise. Orthopaedic Manual Physical Therapy: FROM ART TO EVIDENCE. F. A. Davis Company. 2015.
- Carolyn Kisner, Lynn Allen Colby, John Borstad. Therapeutic exercise : foundations and techniques, Seventh edition. F.A. Davis Company. 2018







